Mark Humayun, MD, PhD, was recently featured on Trailblazers, an original podcast hosted by former CNN chairman and CEO Walter Isaacson. The Trailblazers podcast features leaders across society who have shaken up their fields, innovated in ways many would think impossible and charged forward to pioneer changes that excite the way our world operates. Isaacson, who has written best-selling books on innovators ranging from Leonardo da Vinci to Steve Jobs, sat with Humayun to discuss his career as a world-renown ophthalmologist and inventor. The episode highlights the challenges and victories Humayun has encountered along his journey to reverse blindness and restore a glimmer of hope to vision loss patients living in complete darkness.
Isaacson opens the podcast episode, entitled “Eyesight: Vision’s Visionaries,” with the story of Humayun succeeding in his first attempt to use electrodes to stimulate vision during eye surgery. He recounts the miraculous moment in 1992 when Humayun confirmed that his patient, blind for 50 years, was able to see a small but encouraging flicker of light while lying on the operating table. That light, which his patient described as looking like “a candle far off in the distance on a dark night,” marked a turning point in Humayun’s career and a monumental step forward in the field of vision science.
Almost three decades later, Humayun continues to pioneer groundbreaking advancements in ophthalmology and vision restoration. Humayun is widely recognized for his invention of the world’s first artificial retina, which has restored partial vision to hundreds of patients who were previously completely blind. Humayun and his team continue working to surmount the challenges of recreating one of our most sophisticated senses using a network of electrodes, and their current studies are focused on increasing clarity and adding color vision to their artificial sight system. But perhaps the truest measure of Humayun’s success as a trailblazer lies in the most basic and human experiences his patients have regained thanks to their implants: patients often share stories of watching fireworks on the Fourth of July, appreciating the lights on a Christmas tree, or experiencing the joy of playing with their young grandchildren thanks to the gift of sight their implants have given them.
“Everyone said, ‘This cannot happen,’” Humayun explains on Trailblazers, referring to the many obstacles that complicate creating a bionic eye implant, such as the delicacy of the human retina and the challenge of developing an electrode array capable of creating signals that the human brain can discern as meaningful images. “This was actually science fiction,” Humayun surmises, “and we made it science reality.”
To listen to the full podcast episode, click here.
The Argus II retinal prosthesis––often referred to as the world’s first “bionic eye” ––revolutionized the treatment of blindness. Throughout the past decade, this artificial retina, developed by Mark Humayun, MD, PhD and colleagues in collaboration with Second Sight Medical Products, has enabled hundreds of patients around the world with complete retinal blindness to regain partial eyesight.
The Argus II retinal prosthesis enables patients with complete retinal blindness to see the shapes of objects in their surroundings, such as this Fourth of July fireworks show.
The invention currently allows for black-and-white vision and particularly helps patients detect boundaries between objects in their surroundings. Using a combination of patient feedback and laboratory experiments, Humayun and his team at the USC Dr. Allen and Charlotte Ginsburg Institute for Biomedical Therapeutics continue to enhance the visual information retinal prostheses can offer patients.
In their latest work, USC Ginsburg Institute scientists, in collaboration with USC Institute for Technology and Medical Systems (ITEMS) engineers, have developed detailed computer models of the retina that enable them to test modifications to the prosthetic system with unprecedented ease and speed. These advances in computational modeling have enabled the team to make profound strides forward in understanding how to refine and build upon the device’s capabilities––with the long-term goal of restoring color vision and more precise visual details to patients with progressive blindness.
A look inside the “bionic eye”
At the most basic level, retinal prostheses work by converting visual information from the environment into electrical impulses that stimulate the otherwise blind retina. When these signals reach the vision center of the brain, known as the visual cortex, patients are able to perceive images and shapes from their surroundings.
The Argus II system involves a retinal implant––or, more specifically, a microelectrode array that sits atop and stimulates the retina––coupled with a pair of glasses outfitted with a camera that transmits signals to the implant. When the implant receives visual cues from the camera, it generates small electrical impulses that stimulate the patient’s retinal cells. This stimulation causes the patient to perceive a flash of light that vision scientists refer to as a phosphene.
Image of the Argus II retinal prosthesis, composed of a microelectrode array with thin projections that electrically stimulate the retina.
Phosphenes should ideally appear as small, rounded dots when a single electrode stimulates the retina. In practice, however, patients sometimes perceive a dash instead of a dot––and the reason has to do with the way cells intermesh in the retina.
One of these cell types is the retinal ganglion cell, which plays an essential role in sending visual information from the eye to the brain. Retinal ganglion cells have rounded bodies with many thin projections branching off in different directions and one long projection that feeds information to the brain. These projections overlap and intertwine like the branches of trees in a densely wooded forest, so that when an electrode stimulates one of the retinal cells it often activates the projections of neighboring cells as well.
Example of a retinal ganglion cell, composed of a rounded, central body with numerous small projections and one long projection, or axon, that communicates with the brain (red). Vision scientists at the USC Ginsburg Institute are developing techniques to activate the bodies of specific cells without stimulating the projections of nearby cells, which will help sharpen the visual information that retinal prosthetics can offer patients.
When electrical signals from the prosthesis stimulate both cell bodies and projections from nearby cells, patients perceive a dash of light, called an elongated phosphene, instead of a discrete dot. Humayun’s team set out to determine how to prevent elongated phosphenes from forming so patients could enjoy more refined, detailed vision. Doing so required devising an approach to target retinal cell bodies without activating neighboring cells in the process.
Computer models probe deeper into cellular behavior
To solve this challenge, the USC Ginsburg Institute and USC ITEMS teams first developed computational models to recreate different types of retinal ganglion cells and the patterns in which they overlap. Their models accounted for the relevant functional properties of retinal ganglion cells and could therefore respond to stimuli in ways that mimicked how real retinal ganglion cells would respond. Using these model systems, the scientists ran through a gamut of simulations to find a stimulation pattern that activated cell bodies while avoiding the large projections, known as axons, that other cells use to send visual information to the brain.
In one recent study, the team reported their discovery that very short-duration electrical pulses, as brief as 0.1 milliseconds, can selectively target the intended retinal ganglion cells’ bodies without activating their axons. Their models also enabled them to more accurately map out patterns of cellular activation that arise when shorter pulses are used to stimulate the retina. The researchers hope these, and future, findings can help resolve the problem of elongated phosphenes to ultimately offer patients enhanced visual resolution with a retinal prosthesis.
USC Ginsburg Institute and USC ITEMS scientists are also currently using their computational models of the retina to study possible ways of programming additional visual components, such as color, into the Argus II system. A 2020 study of theirs showed that a particular subtype of retinal ganglion cell, called a bistratified cell, is more responsive to high frequency stimulation than one of its counterparts known as a monostratified cell. Understanding these types of slight differences in responses may help the team improve the performance of retinal prosthetics to enable patients to detect color, contrast and edges of objects. Such research is still ongoing, but based on their preliminary findings, the team is hopeful for the ways they can continue enhancing visual perception for the hundreds of retinal prosthesis users who once lived in complete darkness.
Javad Paknahad, a PhD candidate at USC and the lead author on the aforementioned studies, emphasized how the “multi-scale” nature of these models, which account for the properties of single cells as well as the behavior of entire cell populations, makes this approach particularly valuable. He added that using computer models to study the retina allows their team to run experiments more efficiently, which ultimately accelerates scientific progress. “These multi-scale computational models end up saving a lot of time when doing experiments, because as you continue refining the model system and designing the right programs, you can more readily determine the best approaches to solving complex problems,” he said. “This makes computational modeling very powerful.”
Disclosure: Mark Humayun, MD, PhD, is a co-inventor of the Argus implant series. He is a minority equity owner in Second Sight Medical Products, Inc. and receives royalty payment.
Disclosures: Regenerative Patch Technologies LLC was founded by Mark Humayun, MD, PhD, and David R. Hinton, MD, from the University of Southern California, and Dennis O. Clegg, PhD, from the University of California, Santa Barbara. The technology to produce the stem cell–based retinal implant is exclusively licensed to Regenerative Patch Technologies LLC from the University of Southern California, the California Institute of Technology and the University of California, Santa Barbara. Humayun has an equity interest in and is a consultant for Regenerative Patch Technologies LLC.
Mark Humayun, MD, PhD, was included in a recent analysis out of Stanford University highlighting the world’s leading scientists across 22 fields of research and 176 sub-fields. Within the category of “ophthalmology & optometry,” Humayun ranks among the top 0.2% of his peers.
A recent Stanford study ranked Mark Humayun, MD, PhD, as one of the world’s top scientists. (Image credit: Jill Greenberg)
The rankings were calculated based on metrics such as the number of times a scientist’s research has been cited throughout the individual’s career. The analysis also accounted for each person’s h-index score, which attempts to quantify the scientist’s research productivity balanced with the impact that the research has made on the scientific field.
Humayun, a vitreoretinal surgeon and prolific inventor of biomedical devices, is widely known for developing the world’s first artificial retina. In 2016, Humayun received the National Medal of Technology and Innovation from President Barack Obama for developing the Argus II retinal prosthesis, which restores partial vision to patients with total retinal blindness.
Some of Humayun’s other accolades include election to both the National Academy of Medicine (NAM) and National Academy of Engineering (NAE), the 2020 Medal for Innovations in Healthcare Technology from the Institute of Electrical and Electronics Engineers (IEEE), “Inventor of the Year” from R&D Magazine in 2005, and distinction as one of the top 1% of ophthalmologists in U.S. News & World Report.
Humayun currently serves as director of the USC Dr. Allen and Charlotte Ginsburg Institute for Biomedical Therapeutics and co-director of the USC Roski Eye Institute. He also holds the titles of University Professor and Cornelius J. Pings Chair in Biomedical Sciences at USC.
On November 20th, 2020, the USC Dr. Allen and Charlotte Ginsburg Institute for Biomedical Therapeutics awarded its inaugural Mordechai “Mort” Arditti Award for Excellence to Alejandra Gonzalez-Calle, PhD, a postdoctoral researcher working to develop vision science innovations at the USC Ginsburg Institute.
Dr. Alejandra Gonzalez-Calle, the inaugural recipient of the Mordechai “Mort” Arditti Award for Excellence
Gonzalez-Calle grew up in Medellín, Colombia, and earned a BS in biomedical engineering at La Escuela de Ingenieria de Antioquia. As an undergraduate student, she planned to dedicate her career to developing affordable prosthetic limbs. After an accident that caused her to lose vision in her right eye, however, she redirected her energy toward advancing the field of vision science.
In 2009, Gonzalez-Calle reached out to Mark Humayun, MD, PhD, with the hope that she could pursue a research internship at his team’s USC lab. Humayun and his colleagues had an impressive record of churning out engineering-based solutions to address the biological anomalies causing vision loss, and Gonzalez-Calle aspired to join the ranks of this innovative team. That internship ultimately blossomed into over a decade and counting of collaboratively pioneering interdisciplinary, translational approaches to address some of the most confounding challenges in vision science. During that time, Gonzalez-Calle received one of the USC Viterbi School of Engineering’s highest research awards to support her pursuit of a master’s degree in biomedical engineering, and she later went on to earn a PhD in biomedical engineering in 2017.
Some of Gonzalez-Calle’s most meaningful experiences working with the USC Ginsburg Institute team include fine-tuning the Argus II retinal prosthesis to restore eyesight to patients suffering from complete retinal blindness and contributing to the development of a novel stem cell-based retinal implant for patients with AMD. Recently, she worked with a multidisciplinary team that was able to demonstrate, for the first time, that noninvasive electrical stimulation could be used to slow retinal degeneration in pre-clinical models.
Throughout the years spent working on these remarkable feats in biomedical engineering, Gonzalez-Calle has remained continuously inspired by seeing how the projects to which she has contributed can tangibly enhance patients’ lives. “Being able to see our projects evolve from the basic research stage to the point where they are implanted in patients, and then ultimately seeing how much of a difference these interventions can make in patients’ lives, is what makes me so passionate about what I’m doing,” Gonzalez-Calle says.
Receiving the inaugural Mordechai Arditti Award for Excellence carries special meaning for Gonzalez-Calle due to the fact that the late Arditti was an important mentor of hers throughout her training. Arditti, an electrical engineer by training, often contributed to and enhanced Gonzalez-Calle’s projects by helping to build circuits and essential electrical components of the biomedical devices on which Gonzalez-Calle worked. “He was such a special person for all of us,” Gonzalez-Calle remembers. “Besides being a mentor, he was also a friend to all the PhD students. I’m very grateful to receive this award and to feel like it’s coming from him, even though he’s not here with us anymore.”
An interdisciplinary team of researchers at the University of Southern California has developed a precision drug delivery tool to selectively treat areas of the brain damaged during a traumatic brain injury (TBI). The researchers anticipate that their rapidly deployable intervention could potentially help prevent long-term brain damage in the millions of Americans who sustain a TBI each year.
The effects of TBIs on the American populace are nothing short of staggering. TBIs annually cause more deaths and lifelong disabilities than HIV/AIDS, breast cancer, multiple sclerosis and spinal cord injuries combined. Approximately one third of patients die due to secondary complications related to their TBIs, and in 2014, an average of 155 Americans died following a TBI each day. To compound this dramatic human toll, the economic burden of treating TBIs and their long-term side effects is estimated to be $60-76.5 billion each year.
The causes of TBIs range from falls and forceful sports collisions to car accidents and severe blows to the head. Side effects vary widely, from cognitive challenges and dizziness to emotional changes and depression that can endure for days, weeks, or even years after the initial trauma. If effective treatments are not rapidly deployed, a TBI can trigger biochemical changes and inflammatory responses that progressively worsen a patient’s brain damage. To prevent serious side effects, doctors recommend that patients receive treatment within the “golden hour” after sustaining the injury.
Despite the pressing need for effective and rapidly deployable therapies, there are currently no FDA-approved treatments specifically designed for TBIs. Some existing treatments rely on locating the injury within the skull and assessing the damage before proceeding, but this approach can rob precious time from clinicians attempting to stave off permanent brain damage.
A nanoscale solution to a widespread problem
An ideal treatment approach for TBIs would involve a fast-acting, safe, transportable and easily administered drug that could permeate the brain’s protective barrier at the site of damage. A team of USC scientists, led by researchers at the USC Dr. Allen and Charlotte Ginsburg Institute for Biomedical Therapeutics, has mobilized to meet this urgent clinical need: they recently developed a novel drug delivery tool designed to safely and rapidly treat regions of the brain damaged during a TBI.
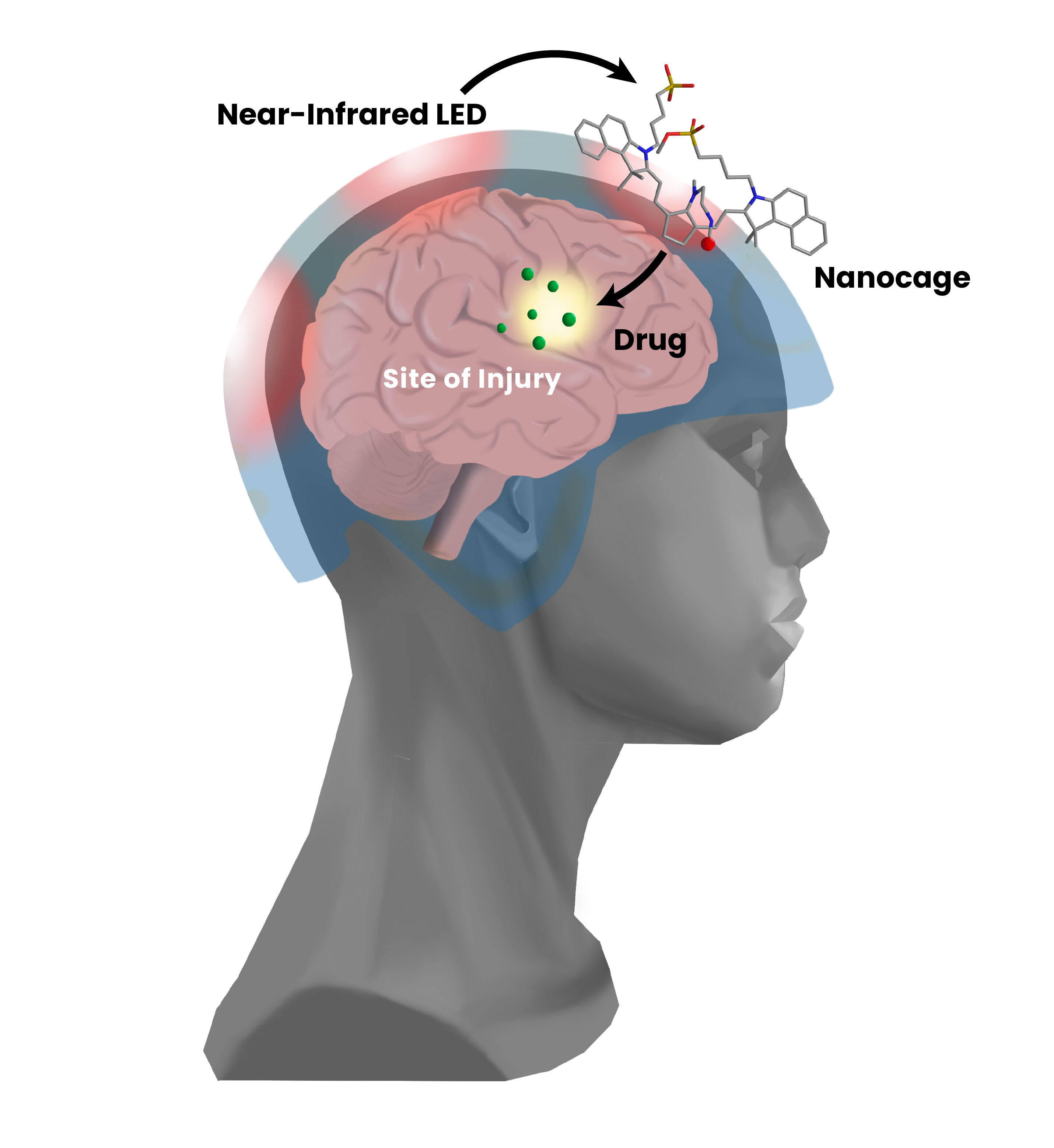
The tool itself is known as a nanocage. As the name suggests, this nanoscale drug carrier works by caging therapeutic agents—in this case, drugs such as gabapentin and cyclosporine A—to carry them within the body. Once a caged drug has migrated through a patient’s circulatory system and made its way to the brain, doctors can beam near-infrared (NIR) light through the patient’s skull to energize the molecule and “open” the cage.
USC scientists have developed an experimental precision treatment for traumatic brain injury (TBI) that involves trapping therapeutic drugs in nanocage carriers before administering treatment. Near-infrared (NIR) light can safely penetrate the skull, and it can be used to “open” the nanocage to release drugs at the site of brain injury. (Image credit: Emily Louie)
The beauty of this approach is multifold. Caging the drug before releasing it at the site of injury minimizes the side effects that one would expect from delivering an active drug throughout the entire body. Moreover, because the brain’s barrier is weakest where it experienced the most trauma, higher concentrations of the drug will enter the brain precisely at the site of damage—thus circumventing the need for time-consuming imaging to locate the damage before proceeding with first-line treatment.
The researchers chose NIR frequency specifically for its ability to safely permeate human tissue without residual side effects, and they designed the nanocage itself to be biodegradable and nontoxic. This emerging intervention is still in its preclinical stages, but the researchers anticipate that it can be packaged as a portable intervention for first responders to immediately administer within a patient’s “golden hour.”
“I’m very hopeful for the impact this drug delivery tool could ultimately have on the millions of patients who experience TBIs each year,” said Mark Humayun, MD, PhD, director of the USC Ginsburg Institute for Biomedical Therapeutics, who is the study’s principal investigator. “A rapid intervention like this could significantly improve patient outcomes, and our team is excited to continue testing this approach to hopefully bring it to the clinic soon.”
Caroline Black, PhD, lead author on the study, says this research was made all the more meaningful because of her personal connection to TBI within her family. “My dad had a severe TBI when he was 17 and I’ve seen how the effects of secondary injury can persist decades after the initial trauma,” said Black, who is a USC-AbbVie postdoctoral fellow specializing in drug delivery sciences at the biopharmaceutical company AbbVie. “Our drug delivery tool has the potential to open new possibilities for rapid treatment of TBI, and I’m excited to see the impact it could have on improving patient outcomes.”
In addition to Humayun and Black, other researchers on the study include Caitlin M. DeAngelo, PhD, of the USC Department of Chemistry; Eugene Zhou and Isaac Asante, PhD, of the USC School of Pharmacy; Stan G. Louie, PharmD, of the USC School of Pharmacy and the USC Dr. Allen and Charlotte Ginsburg Institute for Biomedical Therapeutics; and Nicos A. Petasis, PhD, of the USC Department of Chemistry, the USC School of Pharmacy and the USC Ginsburg Institute.
Vitreoretinal surgeons Amir Kashani, MD, PhD (left) and Mark Humayun, MD, PhD (right) pioneered a new surgical procedure to treat dry age-related macular degeneration.
Dry age-related macular degeneration (dry AMD) poses a significant clinical challenge. It is one of the leading causes of progressive blindness, robbing millions of people over the age of 65 of their central vision, and it often hinders patients’ abilities to read books, drive and discern the faces of their loved ones. Although vitamin-based supplements may slow progression, no treatments currently exist.
A team of physicians and scientists at the USC Dr. Allen and Charlotte Ginsburg Institute for Biomedical Therapeutics (Ginsburg Institute) saw in this situation an opportunity to innovate and pioneer a novel treatment approach for dry AMD patients. Theirs has been a feat of scientific and surgical prowess, and over a decade of their diligence and ingenuity has resulted in what may become the first FDA-approved treatment to transform the prospects of regaining vision for millions of patients.
The Ginsburg Institute team, led by vitreoretinal surgeons Amir Kashani, MD, PhD, associate professor of ophthalmology at the Keck School of Medicine, and Mark Humayun, MD, PhD, director of the Ginsburg Institute and co-director of the USC Roski Eye Institute, developed a stem cell-based retinal implant and accompanying surgical procedure to help restore vision to dry AMD patients. Their innovative approach and insights from their phase 1/2a clinical trial are described in the latest print issue of the American Academy of Ophthalmology’s journal Ophthalmology Retina.
DESIGNING THE IMPLANT
The team accomplished a remarkable multi-part feat that required inventiveness at every turn, starting with designing the novel retinal implant. Dry AMD causes a single layer of cells in the retina called the retinal pigment epithelium (RPE) to deteriorate. The Ginsburg Institute team decided to utilize stem cells to grow RPE tissue in the lab, with the ultimate goal of implanting those cells in patients’ eyes to slow or reverse the damage. Other scientists had attempted to inject stem cell-derived RPE cells into the retina, but had trouble getting the cells to evenly disperse; the Ginsburg Institute scientists instead created a thin membrane made of parylene on which to grow the cells in a single, even layer. Once they had created this RPE layer, the next challenge was to successfully implant it in the eye.
“In practice, being able to get underneath the retina, which is only about a quarter of a millimeter thick, to physically replace the RPE cell layer is a challenging task,” explains Kashani, who is lead author of the publication. “Normally we don’t operate underneath the retina. It’s a place you generally try to avoid during surgery, so that has been a very novel, challenging aspect of delivering these stem cells.”
There are very few tools for performing surgery within the subretinal space. Most available tools were designed 30 to 40 years ago, are relatively bulky and are generally meant to remove scar tissue or other lesions rather than insert anything into the subretinal space. The Ginsburg Institute team decided that the most promising option was to start fresh and design a brand-new tool to fit their purpose.
ENGINEERING THE TOOL
This new tool had to fit a number of criteria: it needed to be made of completely non-toxic materials so as not to harm patients, its design had to be easily reproducible, and it had to be small enough—on a scale of millimeters—to perform minimally invasive surgery inside the eye but large enough to prevent crushing the tissue implant it was meant to deliver.
The surgeons worked with materials and design engineers at the Ginsburg Institute to create single-use forceps with an internal compartment to encapsulate the implant and a roller-style thumbwheel to deploy it. The implant itself is shaped much like a champagne bottle, and the forceps grab onto the narrow end. Rolling the implant into the device’s compartment causes it to fold into a curved shape, and the surgeon can ultimately release it to lay flat inside the eye.
PIONEERING THE SURGICAL TECHNIQUE
With the new instrument and implant came an entirely novel surgical approach. Kashani and Humayun needed to figure out how to create space for the implant in the location of geographic atrophy, which is what doctors call the area of tissue degeneration. To do so, the surgeons decided to create an artificial retinal detachment using a technique called bleb formation, in which a small pocket of space is formed under the retina. “Normally we treat retinal detachments, we don’t make them. In this particular case, we had to create a very well-controlled retinal detachment within an area of scar tissue that is very adherent to the surroundings,” says Kashani. “The challenge was to separate it without damaging the retina.”
In pre-clinical models, creating a bleb alone proved insufficient; the surgeons had to innovate again and ultimately used water pressure to dissect one cell layer from another in a process called targeted hydrodissection. To monitor progress during surgery and prevent complications, the team utilized an advanced imaging technique called optical coherence tomography (OCT) to visualize the dissection at the cellular level. “One part of our job was to make this a very doable surgery and I think we have achieved that with this study,” Kashani says.
“Without tools like OCT, it would be very difficult to visualize the damage we need to treat,” Kashani explains. He emphasizes that in addition to using OCT intraoperatively, he sees a promising role for the technology to be used in earlier-stage AMD patients to monitor the progression of their geographic atrophy. “It’s not a standard of practice to use OCT and other diagnostic methods to detect early and subtle disease changes, but that may prove to be really important for classifying disease and treating it in the future.”
Kashani adds that one of the most rewarding aspects of the entire clinical trial process has been working with his patients and witnessing their commitment to making this translation from research lab to clinical practice possible. “None of this is happening by magic. Patients are volunteering, and they’re taking a chance for the sake of advancing medicine and potentially helping countless other patients down the road. We always appreciate that effort and we thank the patients and their families, too.”
––
This phase 1/2a trial was supported in large part by a $3.73 million grant from the California Institute for Regenerative Medicine (CIRM). Other authors on the study include Jeremy Uang, BS, of the USC Roski Eye Institute, USC Ginsburg Institute for Biomedical Therapeutics and Department of Ophthalmology, Keck School of Medicine of USC; Melissa Mert, MS, of the Southern California Clinical and Translational Science Institute and USC Department of Preventive Medicine (Biostatistics); Firas Rahhal, MD, of the Retina-Vitreous Associates Medical Group; Clement Chan, MD, of the Southern California Desert Retina Consultants, Palm Desert; Robert L. Avery, MD, of the California Retinal Consultants, Santa Barbara; Pravin Dugel, MD of the Retinal Consultants of Arizona, Phoenix; Sanford Chen, MD, of Orange County Retina, Santa Ana; Jane Lebkowski, PhD, of Regenerative Patch Technologies LLC; Dennis O. Clegg, PhD, of the center for Stem Cell Biology and Engineering, University of California; and David R. Hinton, MD, of the Department of Pathology, Keck School of Medicine of USC.